
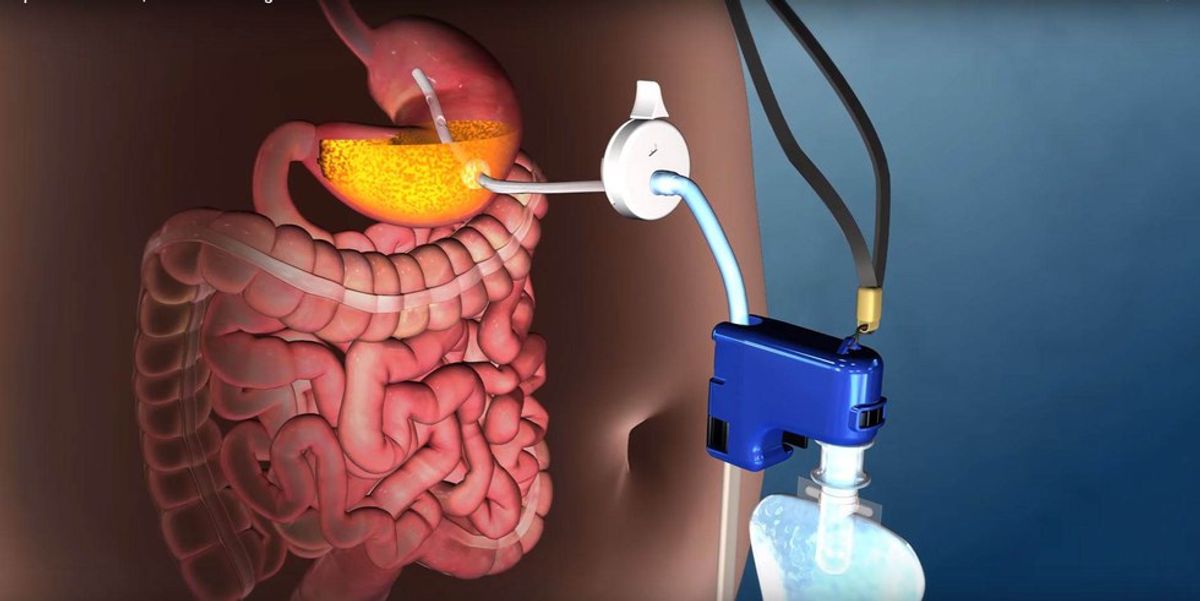
On June 14th, 2016, the Food and Drug Administration approved a new, highly controversial weight loss device that functions by allowing the user to "pump and dump" about one-third of their stomach contents straight into the toilet. The device includes a tube that goes from the inside of the stomach running to a port on the outside of the body. The pump itself can be attached to the outside port as needed to remove stomach contents.
Clinical trials indicate that the pump is considerably effective with weight loss: The average patient saw a loss of 46 pounds lost in the first year and 50 pounds in the following year. However, the good press gave no mention of their change in critical nutritional markers such as electrolyte, vitamin and mineral levels. These levels could be expected to be off kilter as a result of side effects such as vomiting and diarrhea over a sustained period of time. Either of these bodily functions, even in the short term, can cause dehydration, throwing off an individual's electrolyte balance.
"The AspireAssist device should not be used on patients with eating disorders, and it is not intended to be used for short durations in those who are moderately overweight," the FDA said in a statement.
In my estimation, the lack of judgment and foresight in this approval is irresponsible beyond reason. This is not a gray area. This is crossing the line from medical intervention and "assistance" into the territory of enabling disordered behavior and purging pathology.
Others have made mention that the process smacks of "assisted bulimia" as well.
In defense of the opprobrium, Dr. Shelby Sullivan of Washington University in St. Louis, who helped test the AspireAssist said:
"There is no such thing as medical bulimia or assisted bulimia. Bulimia is an eating disorder defined by overeating and then purging, often though forced vomiting. Patients eat less with this therapy then they did before.
People think patients can eat whatever they want and then aspirate it and that's just not true.
It has to be liquid enough and the particles have to be small enough to get through the tube."-NBC News
When I read her rebuttal, I literally felt sick.
This is forced purging calories after eating, is it not?
And the fact of the matter is, most obese patients--and candidates for this type of elective procedure-- are compulsive overeaters. Obesity disease is real, but it is rare.Most, I say, most obese patients are binge eaters in the habitual and pathological sense.
Because this medical intervention can be looked at as a "quick fix" and not necessarily a lifestyle change, most patients will not be deterred from continuing to eat in the quantities in which they are accustomed. What I have just described to you is binge eating disorder as qualified in the DSMV.
Compulsive overeaters and Binge eaters (those with Binge Eating Disorder) are actually quite similar to bulimics in that they both typically consume large amounts of food privately, in a discrete period of time.
In this particular Q & A, although Sullivan implies they are not, many potential candidates for AspireAssist are, in fact, eating disordered because they meet the DSMV criteria for Binge Eating Disorder.
I'm curious to know what this medical doctor knows about eating disorders that makes her an authority to make an argument that bulimic behavior is so vastly different from binge eating behavior. I'd also like to know how she thinks AspireAssist's methodology of purging calories bears such little resemblance to purging behavior in bulimia when the food eaten winds up in the toilet either way.
But most of all, and likely, most importantly, on what grounds can she guarantee that the patients won't overeat as they've compulsively and habitually done for long enough to arrive at their weight in the first place?
Those who have established compulsions, obsessions and addictions do not stop behaviors without a multifaceted approach. Inserting a foreign object in an organ will not change the disordered behavior. It will only cause the disordered behavior to adapt, to mutate, so that it may live on and thrive. I know this.
Allow me to provide you a nearly analogous example in the scope of medical intervention concerning obesity:
When many obese patients have received gastric bypass surgery, they have experienced bulimic effects due to the continuation of the same binge-eating compulsions.
However, due to the fact that their stomach now lacks the ability to hold the same large quantity of food in so short a span of time, they find themselves involuntarily regurgitating the food. This happened so often, that the vomiting became habitual and an advantageous part of the process, thus the vicious cycle of bulimia is formed by way of medical intervention.
And this isn't a one-off occurrence. All one has to do is google the words "bariatric" and "bulimia" and their search results will overfloweth.
According to Angela Guarda, director of the Eating Disorders Program at Johns Hopkins Medicine, in 2014 alone, 8 percent of patients admitted to the Johns Hopkins Eating Disorders Program had a history of bariatric surgery. Some patients developed their eating disorder after their surgery, and others had a pre-existing condition that worsened after the procedure.
Janelle Coughlin, the director of obesity behavioral medicine at Hopkins, who also works with the Johns Hopkins Eating Disorder Program, confirmed that binge eating is the root problem prior to surgery. After surgery, physical reality limits the amount one can eat in a sitting, but she said that doesn't stop some of them from grazing all day long because the overeating habit is ingrained. Conversely, some develop anorexia or bulimia because they obsess over every calorie or utilize the vomiting after gastric bypass surgery advantageously and habitually.
Sullivan argued that AspireAssist would not lead to bulimia and that there is "no such thing as medically assisted bulimia". She says that by using AspireAssist, patients will reduce their overall intake because the food must be broken down into small enough particles to fit through the tube so it can then be aspirated into the toilet and flushed away. Ok, so...what? Chewing is what I am missing here?
My final thoughts:
It concerns me that one of their lead doctors considers her patients in control of their binge eating to the extent that she wouldn't characterize their eating behavior as disordered, although it is outlined as such by the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders.
Dr. Shelby Sullivan and her team would benefit from looking at the correlation between eating disorders and Bariatric Surgery because they are working with patients within the identical demographic. Arming themselves with the knowledge regarding how some of those situations played out could help them anticipate problems and perhaps even make this device safer and less likely to cause a secondary disorder.
If someone is absolutely required to use such a device for a life-sustaining purpose, say, in the event that they needed it to support their digestive system due to ostomy surgery, then I would be more than supportive. However, this device for weight loss is controversial at best, and dangerous at worst. It is absolutely triggering and harmful to the eating disordered community in all stages of recovery.
Tell me what you think about this controversial new medical intervention!
I'd love to hear about it!


 Going to the cinema alone is good for your mental health, says science
Going to the cinema alone is good for your mental health, says science










 women in street dancing
Photo by
women in street dancing
Photo by  man and woman standing in front of louver door
Photo by
man and woman standing in front of louver door
Photo by  man in black t-shirt holding coca cola bottle
Photo by
man in black t-shirt holding coca cola bottle
Photo by  red and white coca cola signage
Photo by
red and white coca cola signage
Photo by  man holding luggage photo
Photo by
man holding luggage photo
Photo by  topless boy in blue denim jeans riding red bicycle during daytime
Photo by
topless boy in blue denim jeans riding red bicycle during daytime
Photo by  trust spelled with wooden letter blocks on a table
Photo by
trust spelled with wooden letter blocks on a table
Photo by  Everyone is Welcome signage
Photo by
Everyone is Welcome signage
Photo by  man with cap and background with red and pink wall l
Photo by
man with cap and background with red and pink wall l
Photo by  difficult roads lead to beautiful destinations desk decor
Photo by
difficult roads lead to beautiful destinations desk decor
Photo by  photography of woman pointing her finger near an man
Photo by
photography of woman pointing her finger near an man
Photo by  closeup photography of woman smiling
Photo by
closeup photography of woman smiling
Photo by  a man doing a trick on a skateboard
Photo by
a man doing a trick on a skateboard
Photo by  two men
two men  running man on bridge
Photo by
running man on bridge
Photo by  orange white and black bag
Photo by
orange white and black bag
Photo by  girl sitting on gray rocks
Photo by
girl sitting on gray rocks
Photo by  assorted-color painted wall with painting materials
Photo by
assorted-color painted wall with painting materials
Photo by  three women sitting on brown wooden bench
Photo by
three women sitting on brown wooden bench
Photo by 
 Photo by
Photo by  Photo by
Photo by  Photo by
Photo by  Photo by
Photo by 
 people sitting on chair in front of computer
people sitting on chair in front of computer

 all stars lol GIF by Lifetime
all stars lol GIF by Lifetime two women talking while looking at laptop computerPhoto by
two women talking while looking at laptop computerPhoto by  shallow focus photography of two boys doing wacky facesPhoto by
shallow focus photography of two boys doing wacky facesPhoto by  happy birthday balloons with happy birthday textPhoto by
happy birthday balloons with happy birthday textPhoto by  itty-bitty living space." | The Genie shows Aladdin how… | Flickr
itty-bitty living space." | The Genie shows Aladdin how… | Flickr shallow focus photography of dog and catPhoto by
shallow focus photography of dog and catPhoto by  yellow Volkswagen van on roadPhoto by
yellow Volkswagen van on roadPhoto by  orange i have a crush on you neon light signagePhoto by
orange i have a crush on you neon light signagePhoto by  5 Tattoos Artist That Will Make You Want A Tattoo
5 Tattoos Artist That Will Make You Want A Tattoo woman biting pencil while sitting on chair in front of computer during daytimePhoto by
woman biting pencil while sitting on chair in front of computer during daytimePhoto by  a scrabbled wooden block spelling the word prizePhoto by
a scrabbled wooden block spelling the word prizePhoto by 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}